Published
Outcomes of Incidentally Discovered Thyroid Nodules Referred to a High Volume Head and Neck Surgeon
by Teresa R. Kroeker, MD, Gavin le Nobel, MD, Mazin Merdad, MD, Jeremy L. Freeman, MD
Head and Neck. 2013 Jun 1. doi: 10.1002/hed.23273.
The yearly incidence of thyroid cancer is increasing, in part due to detection of non-palpable nodules on ultrasound and cross-sectional imaging performed for unrelated issues. Incidental thyroid nodules are commonly found by radiological studies done for other indications.

Abstract
BACKGROUND
Incidental thyroid nodules are commonly found by radiological studies done for other indications. The yearly incidence of thyroid cancer is increasing in part due to detection of non-palpable nodules on imaging performed for unrelated issues.
METHODS
All new patients referred to a high-volume thyroid surgeon for thyroid nodules were reviewed between February 2009 and January 2011. Data regarding patient demographics, risk factors, referring physician, radiologic findings, fine needle aspiration results, and management were reviewed.
RESULTS
133 of 729 patients (18.2%) had a thyroid nodule or nodules incidentally found on ultrasound, MRI, CT, nuclear imaging, or chest x-ray. Fifty-five (41.4%) patients were managed surgically, with 35 (63.6%) of those having thyroid cancer on final surgical pathology.
CONCLUSION
Based on radiologic findings, risk factors, and fine needle aspiration results, many incidental thyroid nodules can be observed. Incidental thyroid nodules should be evaluated in the same fashion as a palpable thyroid nodule.
*If you would like a PDF file of this full article, please send a request via e-mail to tkroeker.md@gmail.com.
Central Neck Dissection for Papillary Thyroid Cancer
by Jeremy L. Freeman, MD, Teresa R. Kroeker, MD
ENT and Audiology News 21(4):57-59, 2012.

The incidence of papillary thyroid cancer has escalated significantly over the past several decades. The American Cancer Society reports that more than 56,000 new cases were diagnosed in 2012. The death rate, however, has remained the same over the past several decades. Therefore it appears that the increased incidence in no small part is due to increased detection, mostly because of ultrasonographic examination for unrelated reasons and also due to a shifting paradigm in reporting from a pathology perspective. As more cases are presenting to endocrinologists and surgeons, it is incumbent upon them to treat these cases in a rational evidence-based manner, especially with respect to the management of lymph node compartments.
Metastatic Papillary Thyroid Cancer with Lateral Neck Disease: Pattern of Spread by Level
by Mazin Merdad, MD, MPH, Antoine Eskander, MD, Teresa Kroeker, MD, Jeremy L. Freeman, MD
Head Neck. 2012 Sep 10. doi: 10.1002/hed.23149.

Papillary thyroid cancer commonly metastasizes via lymphatic spread to local and regional lymph nodes. A high rate of clinical and occult metastases has been well documented in the literature with a range from 30% to 90%. Lymph node metastases in PTC has a significant impact on disease-free survival and disease specific survival.
Abstract
BACKGROUND
Currently, there is no clear consensus on the extent of this lateral neck dissection required in papillary thyroid cancer (PTC) with lateral neck metastasis. The purpose of this study was to review our experience with metastatic PTC, and identify the pattern of lymphatic spread to the lateral neck.
METHODS
A retrospective medical chart review of PTC patients treated with lateral neck dissection (levels II-Vb) at our institution between January 2004 and 2011. A total of 185 patients underwent 248 selective lateral neck dissections.
RESULTS
Levels II, III, IV, and Vb were respectively involved in 49.3%, 76.6%, 61.6%, and 29.2% of cases.
CONCLUSION
We advocate for a routine excision of levels II, III, IV, and Vb in PTC with metastasize to any lateral neck level. Although we have routinely dissected level IIb, it may be appropriate to omit its dissection, as well as level Va, when there are no clinical, radiologic, or intraoperative evidence of disease involving these sublevels.
*If you would like a PDF file of this full article, please send a request via e-mail to tkroeker.md@gmail.com.
Predictors of Level II and Vb Neck Disease in Metastatic Papillary Thyroid Cancer
by Mazin Merdad, MD, MPH; Antoine Eskander, MD; Teresa Kroeker, MD; Jeremy L. Freeman, MD, FRCSC
Arch Otolaryngol Head Neck Surg. 2012 Nov 1;138(11):1030-3.

Papillary thyroid cancer commonly spreads to regional lymph nodes. Metastasis to the lateral neck largely occurs in a predictable manner, with the middle and lower jugular lymph nodes most commonly involved. Several pathologic factors have been previously shown to have a significant association with lateral neck metastasis in papillary thyroid cancer, including multifocality and thyroid capsular invasion.
Abstract
OBJECTIVE
To identify predictors of levels II and Vb involvement in papillary thyroid cancer (PTC) with lateral neck metastasis.
DESIGN
Large case series.
SETTING
High-volume tertiary care hospital.
PATIENTS
Consecutive sample of 185 patients who underwent 248 selective neck dissections of at least levels II to V for pathologically proven PTC.
MAIN OUTCOME MEASURES
Significant independent predictors of level II and Vb metastasis, including age and pathologic variables (tumor diameter, dominant nodule cellular pathology, multifocality, extracapsular invasion, positive margins, and lymphovascular invasion).
RESULTS
Levels II and Vb were involved in 49.3% and 29.2% of our cohort, respectively. Age and lymphovascular invasion were independent predictors of level Vb involvement with metastasis (logistic regression: odds ratio for age = 0.92, SE = 0.03, P = .02; and odds ratio for lymphovascular invasion = 5.52, SE = 0.80, P = .03). No significant predictors were identified for level II involvement.
CONCLUSIONS
Levels II and Vb were involved in a significant number of patients with PTC and lateral neck disease. Younger age and lymphovascular involvement were independent risk factors for level Vb involvement in patients with PTC and lateral neck metastasis. The increased risk might be of marginal clinical significance. No significant predictors were identified for level II involvement. Our findings do not favor a limited neck dissection on the basis of any of the study’s clinical or pathologic variables, and we therefore recommend the routine excision of levels IIa to Vb in all patients with PTC presenting with lateral neck disease.
*If you would like a PDF file of this full article, please send a request via e-mail to tkroeker.md@gmail.com.
Parathyroid Adenoma on the Ipsilateral Side of Thyroid Hemiagenesis
by Teresa R. Kroeker, MD, Kevin M. Stancoven, MD, and John T. Preskitt, MD
Proc (Bayl Univ Med Cent). 2011 Apr;24(2):92-3.
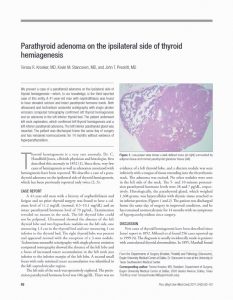
We present a case of a parathyroid adenoma on the ipsilateral side of thyroid hemiagenesis-which, to our knowledge, is the third reported case of this entity. A 41-year-old man with nephrolithiasis was found to have elevated calcium and intact parathyroid hormone levels. Both ultrasound and technetium sestamibi scintigraphy with single photon emission computed tomography confirmed left thyroid hemiagenesis and an adenoma in the left inferior thyroid bed. The patient underwent left neck exploration, which confirmed left thyroid hemiagenesis and a left inferior parathyroid adenoma. The left inferior parathyroid gland was resected. The patient was discharged home the same day of surgery and has remained normocalcemic for 14 months without evidence of hyperparathyroidism.
Outcomes of Combined Oncologic Resection and Carotid Endarterectomy in Patients with Head and Neck Cancer
by Teresa R. Kroeker, MD, John C. O’Brien, MD
Head Neck. 2013 May;35(5):E167-70. doi: 10.1002/hed.22919.

Patients with head and neck cancer have similar risk factors to patients with carotid disease, such as increased age, smoking, hypercholesterolemia, irradiation, hypertension, male sex, and alcoholism. Patients with head and neck cancer should be screened through their medical history, physical examination, and imaging with vascular consultations obtained as indicated. Carotid bruits may be heard on physical examination, calcification may be seen at the carotid bifurcation on imaging studies, and a carotid duplex ultrasound may show elevated arterial velocities. It is uncommon for head and neck surgeons to consider a carotid endarterectomy and oncologic surgery at the same sitting.
Abstract
BACKGROUND
Patients with head and neck cancer have similar risk factors to patients with carotid disease. Patients with head and neck cancer should be screened with vascular consultations obtained as indicated. Identification of significant carotid artery disease before surgical treatment of head and neck cancer is important in order to prevent perioperative and future strokes.
METHODS
Eleven patients underwent carotid duplex ultrasound followed by vascular consultation for significant asymptomatic and symptomatic carotid stenosis. Carotid endarterectomy was performed during an oncologic resection of head and neck cancer between the years of 1996 and 2011.
RESULTS
There were no local or regional recurrences. There were no perioperative deaths or strokes. Two-year and 5-year survival were 70% and 29%, respectively, with a median survival of 51 months.
CONCLUSION
Collaboration of head and neck surgeons with vascular surgeons provides the patient with an oncologic resection and revascularization with a low perioperative risk of stroke. This improves the patient’s quality of life by lessening the possibility of a stroke postoperatively.
*If you would like a PDF file of this full article, please send a request via e-mail to tkroeker.md@gmail.com.
Carotid Resection and Reconstruction Associated with Treatment of Head and Neck Cancer
by Teresa R. Kroeker, MD, and John C. O’Brien, MD
Proc (Bayl Univ Med Cent). 2011 October; 24(4): 295–298.

Patients with head and neck cancer may experience carotid artery involvement. We present a series of 10 patients, all with stage IVB disease, who required carotid resection and reconstruction to achieve a complete resection. Nine of the 10 patients had previous radiation treatment to the neck. Six died of distant disease, and three died of other causes with no local or regional recurrences. Carotid resection and reconstruction can be done safely, achieving local and regional control.